Pancreatobiliary Adenocarcinoma Metastatic To The Liver
A 73 year old woman is presented with abdominal pain, weight loss and weakness. After admission to the hospital, she was found to have pancreatic body mass and multiple liver nodules. One of the nodules was biopsied.



Histology
This is a moderately differentiated adenocarcinoma consisting of tubular and duct-like structures surrounded by desmoplastic stroma and infiltrating normal liver tissue. The neoplastic glands are lined by a single layer of cuboidal pleomorphic cells.
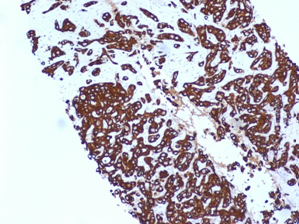
The adenocarcinoma from any organ may look the same and with a help of immunohistochemical stains, the specific primary site may be determined.
The immunohistochemical stains were positive for CK7, CK-17, CK-19, and CA19.9 and consistent with PANCREATOBILIARY ADENOCARCINOMA.
Pancreatic Adenocarcinoma
The etiology is largely unknown. The ductal adenocarcinoma affects both sexes almost equally with its peak incidence in the 6th -7th decades of life and is extremely rare before the age of 40.
There are few risk factors:
- Smoking
- High intake of dietary fat and chronic pancreatitis
- May be associated with some genetic syndromes (familial atypical multiple mole/melanoma syndrome, telangiectatic ataxia and Peutz-Jeghers syndrome)
- Family history
There are no screening tests available
In about two thirds of the patients, the tumor involves the head of the pancreas, causing obstruction of the biliary tract and often also of the pancreatic duct. The patients present with jaundice and weight loss and usually also pain because of the early infiltration of the nerves in the retroperitoneal tissue. In addition, some patients may have recent-onset diabetes and acute pancreatitis.
A third of the patients have the tumor in the body and/or the tail of the pancreas and a minority in the uncinate process. These patients often present with pain and weight loss or liver metastases from an “occult” primary, because the growth of their carcinomas is hardly hindered by any anatomic border and therefore rapidly involves extra-pancreatic tissues (retroperitoneum, peritoneum, stomach, colon, spleen and left adrenal gland).
Prognosis
Most (80-90%) ductal adenocarcinomas are not resectable at the time of diagnosis and the patients rarely live longer than six months. Of the patients with resectable tumor s, approximately 80-90% survive no longer than three years. The five year survival rate after surgery is approximately 15%. However, improved survival data has been reported in some recent series from Japan, the USA and Europe. Local tumor recurrence is common after surgical resection and is one of the factors determining survival.
Case read and contributed by Elena Lavrovskaya, MD.